This week’s image is brought to us by Brooks Moore, Alex Moore, and Gail Ferek. This patient presented to the emergency department for increasing fatigue and shortness of breath. A CXR was obtained which showed a complete white-out of the right lung (See below). The X-ray was read by radiology as “Opacification right chest most compatible with increasing pleural effusion and atelectasis.” Ultrasound can distinguish consolidated lung from effusion and can be essential prior to performing a thoracentesis to determine if there is sufficient fluid to be tapped.

The image below was obtained by placing the curvilinear probe on the lateral aspect of the RUQ with the indicator marker towards the head (similar to obtaining a RUQ FAST exam, but with the probe angled slightly more towards the head to capture more of the lung). We can see the liver outlined by the thin hyperechoic diaphragm. Just superior to this, there is a stripe of anechoic fluid representing a small pleural effusion. Looking further towards the head we see the lung, which in this image has echogenicity similar to that of the liver.

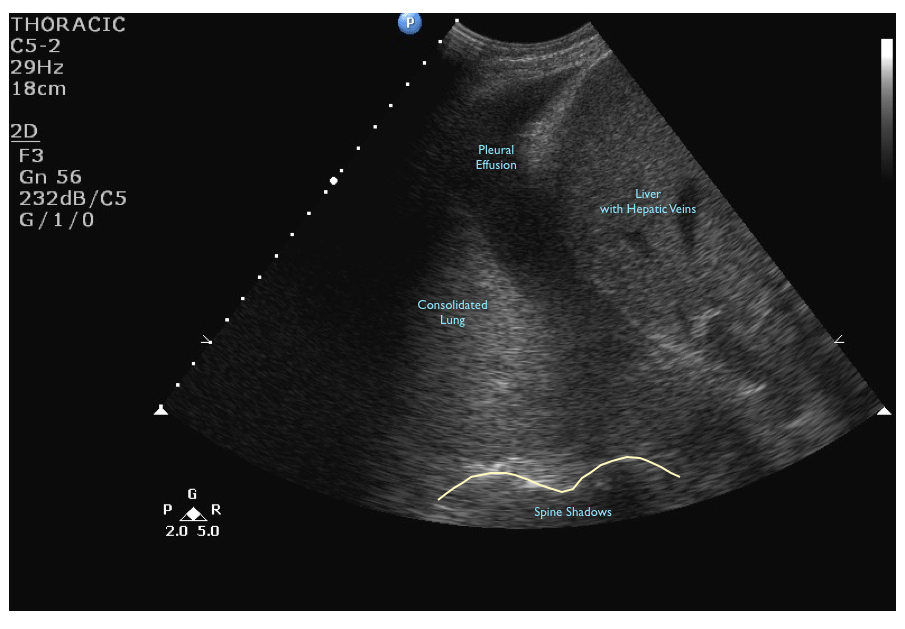
This is the appearance of consolidated lung (in this case, cancer). Normal lung is air-filled and not readily visible with ultrasound, but in consolidation as fluid fills the lung and displaces air the lung is easier to visualize with ultrasound.
In this image its easy to see the difference between collapsed lung (from cancer) and pleural fluid, but in some cases complex effusions can be more difficult to distinguish. You can look for air bronchograms (small bright reflectors from air trapped in the lung), or doppler can be used to visualize small pulmonary vessels.
8/26/2011